


Wolfgang Vogt, MD:
This is completely inexplicable to me because the scale distortions in the shoulder area are immense in X-ray images on transparencies. Because of the images
the different body postures during the X-ray exposures, the
the X-ray images, the resulting considerable size deviations due to the distance to the X-ray film, and the resulting lack of accurate representation of the
bones in the required standard planes, precise size and angle measurement is practically impossible.
is practically impossible. In addition, we now live in
an ever-increasing digital world, planning with normal one-dimensional X-ray images is no longer up to date!
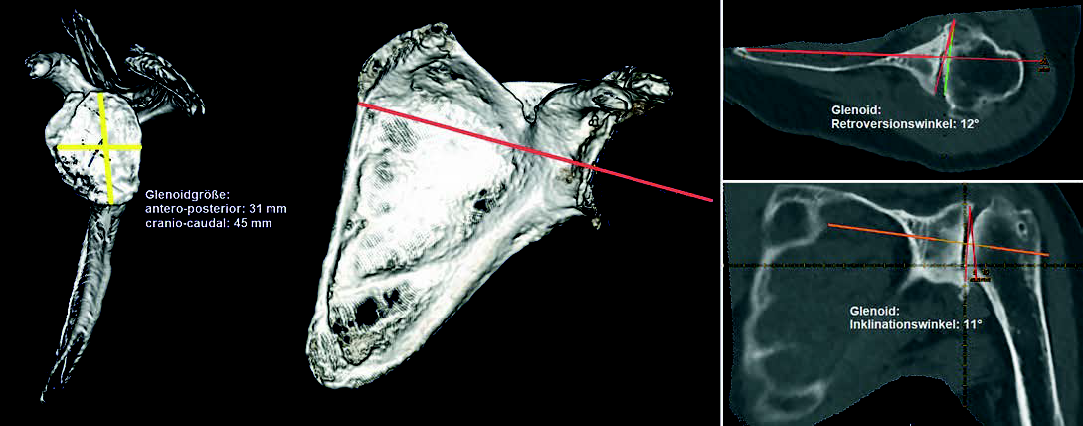

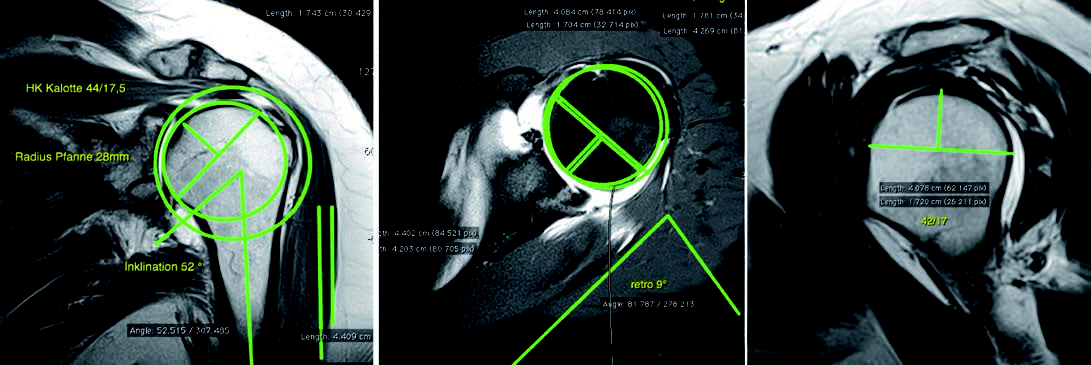
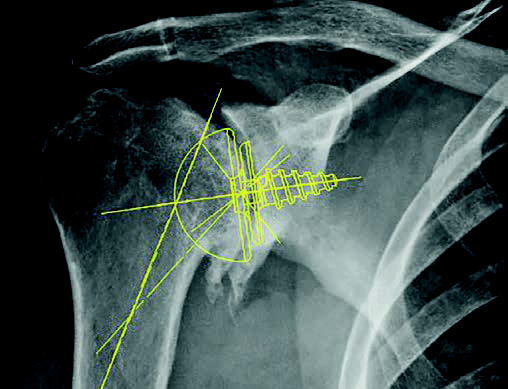
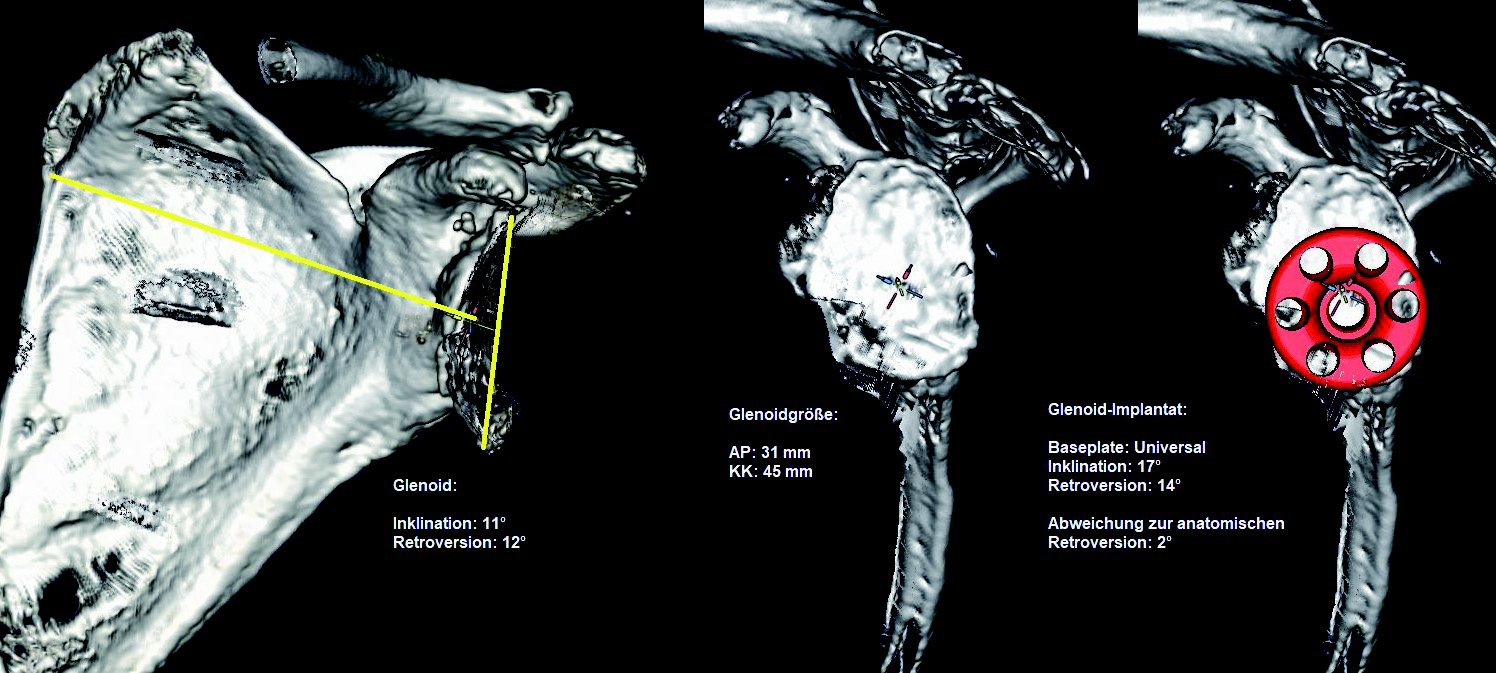
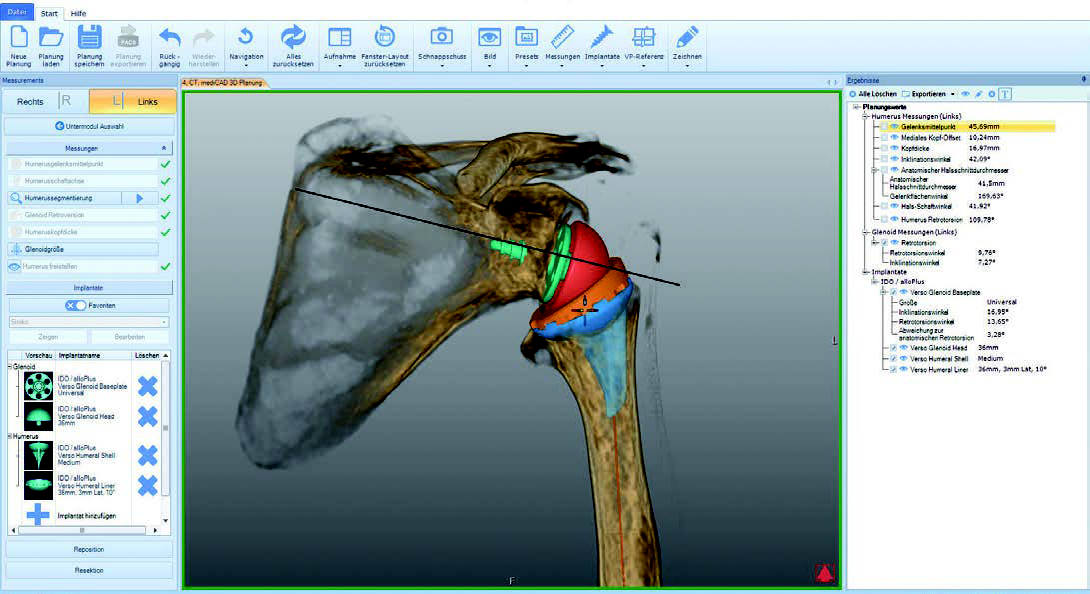
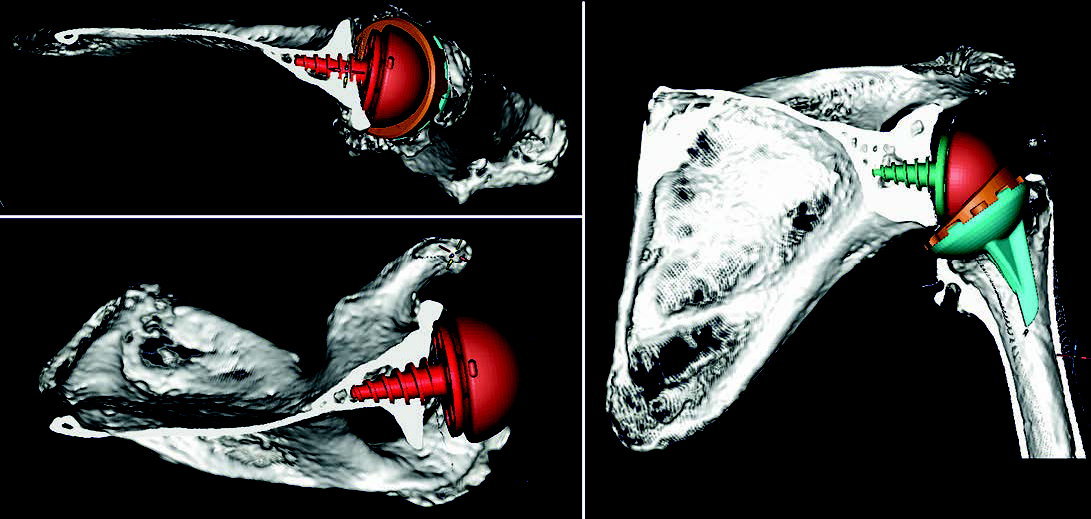
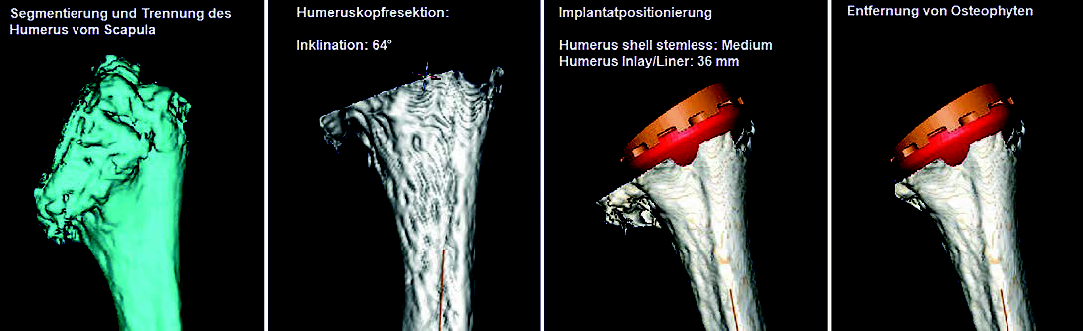
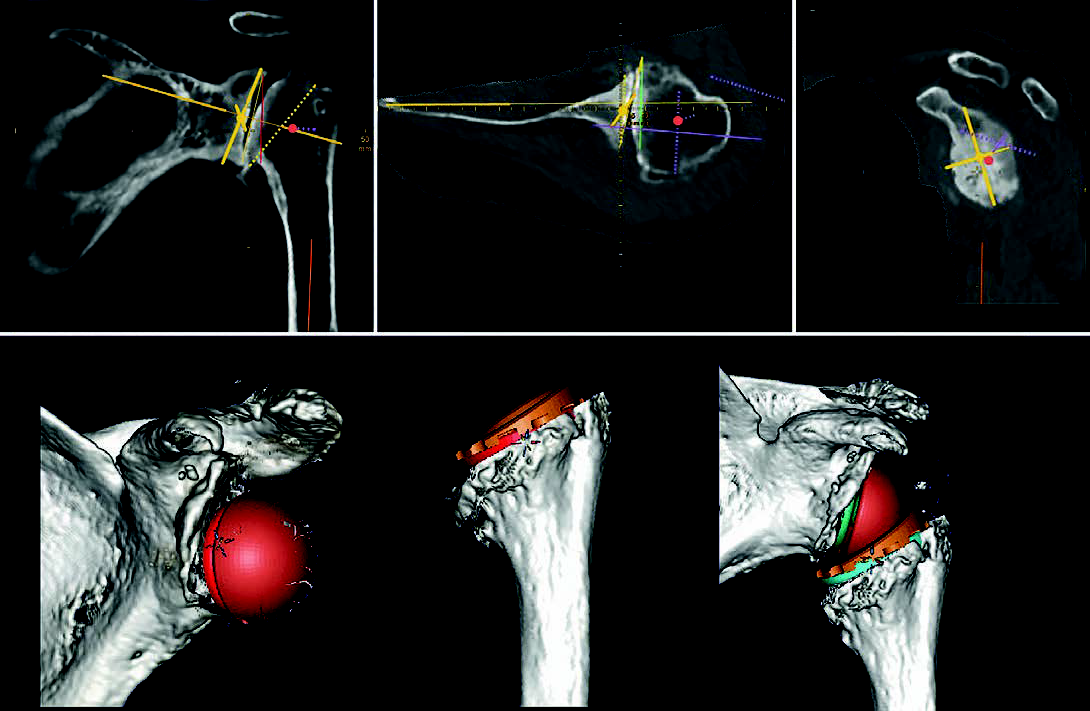
The humeral head resection with the necessary osteophyte resection as well as the positioning of the glenoid component is much easier for me and can be performed more accurately with better knowledge of the size relationships. In the end, this helps the patient because the result in terms of mobility of the shoulder joint replacement and survival time of the prosthesis is better. In addition, I observe a reduction in OR time, the more precise the planning, the less time the patient spends in the OR.


At the OFZ Weilheim – Garmisch – Starnberg – Penzberg, approx. 750 shoulder operations are performed per year, including approx. 100 prosthesis operations. The orthopedic specialist center is a supraregional orthopedic group practice with four practice locations, five cooperating clinics and its own outpatient surgery center as well as a total of 13 specialists in orthopedics, orthopedic and trauma surgery and surgery. The OFZ team “Upper Extremity, Shoulder and Elbow” consists of three colleagues specialized in these sub-specialties: Dr. Wolfgang Vogt, Dr. Johann Wasmaier and PD Dr. Stefan Buchmann.