

Published, 21.10.2022
Is it the “End of an Era” like Riviere et al. claim, which happens now to mechanical alignment in total knee arthroplasty?1)
At mediCAD® we think a lot about how to make the currently 20-30% unsatisfied TKA patients happy, and we know, since results are consistent throughout many countries with sufficient statistics, that there must be a systematic error in the implant alignment technique performed so far. Where can this error be?
There is almost a consensus reached that patellofemoral maltracking is a major cause for the anterior knee pain2);3), which is one of the most common reasons for dissatisfaction among patients, but there appear to be a couple of other factors such as an oversizing of the implants, a wrong rotation in general, a Patella baja and other ligamentous factors impacting negatively TKA patients’ satisfaction.4)
All these factors will never be eliminated in the scope of a traditional mechanical alignment approach planned on an AP x-ray under weight-bearing conditions as followed since the very start of TKA. And a longer lifetime of the implant assured by mechanical alignment should not convince us of the opposite.5)
Correcting the leg axis not entirely for patients with strong Varus/Valgus deformities one could account for ligament laxities already much better than systematically correcting all patients to the WBA, which introduced a more patient-specific approach to TKA firstly.6)
Anatomical alignment as introduced in the 1980s by Hungerford et al. to improve functionality by closer mimicking the native knee alignment was another approach towards a better outcome in TKA, but again relied on a systematic approach, since anatomic alignment aims for a neutral HKA, but the bones are cut 3° oblique to their mechanical axes to reflect the population’s mean native joint line orientation (3° femoral valgus and 3° tibial varus).7) Nowadays this approach is incorporated in the implant design of numerous manufacturers.
Lately, however, with the advent of several PSI (Patient-specific instrumentation/implantation) solutions for TKA on the market, such as Visionaire, myKnee or TruMatch which are growing their market share, a more and more patient-specific approach cannot be neglected anymore and is increasingly replacing the systematic approaches. All the mentioned PSI solutions require 3D data in the form of CT or MRI scans to build their instrumentation kit.8)
Most of the PSI solutions move the responsibility of preoperative planning from the surgeon to a private company providing a service to the hospital. This has long been considered to interfere too much with the codex as agreed upon by many key opinion leaders in the field of orthopedic surgery and traumatology.
Only proper planning executed by the surgeon in charge of operating on their patients should be accepted by the patient and this is what the 3D-planning of mediCAD wants the surgeon to be able to do. Keep the planning in your hands because 3D-planning allows you to follow any desired alignment technique.
Be it that you want to follow the knee phenotypes for your alignment technique proposed by Hirschmann et al.9) or you want to follow the restricted kinematic workflow 10). You can pursue an individual approach when planning your TKA and do not have to rely on the work of a private company whose result you are ultimately held to account for.
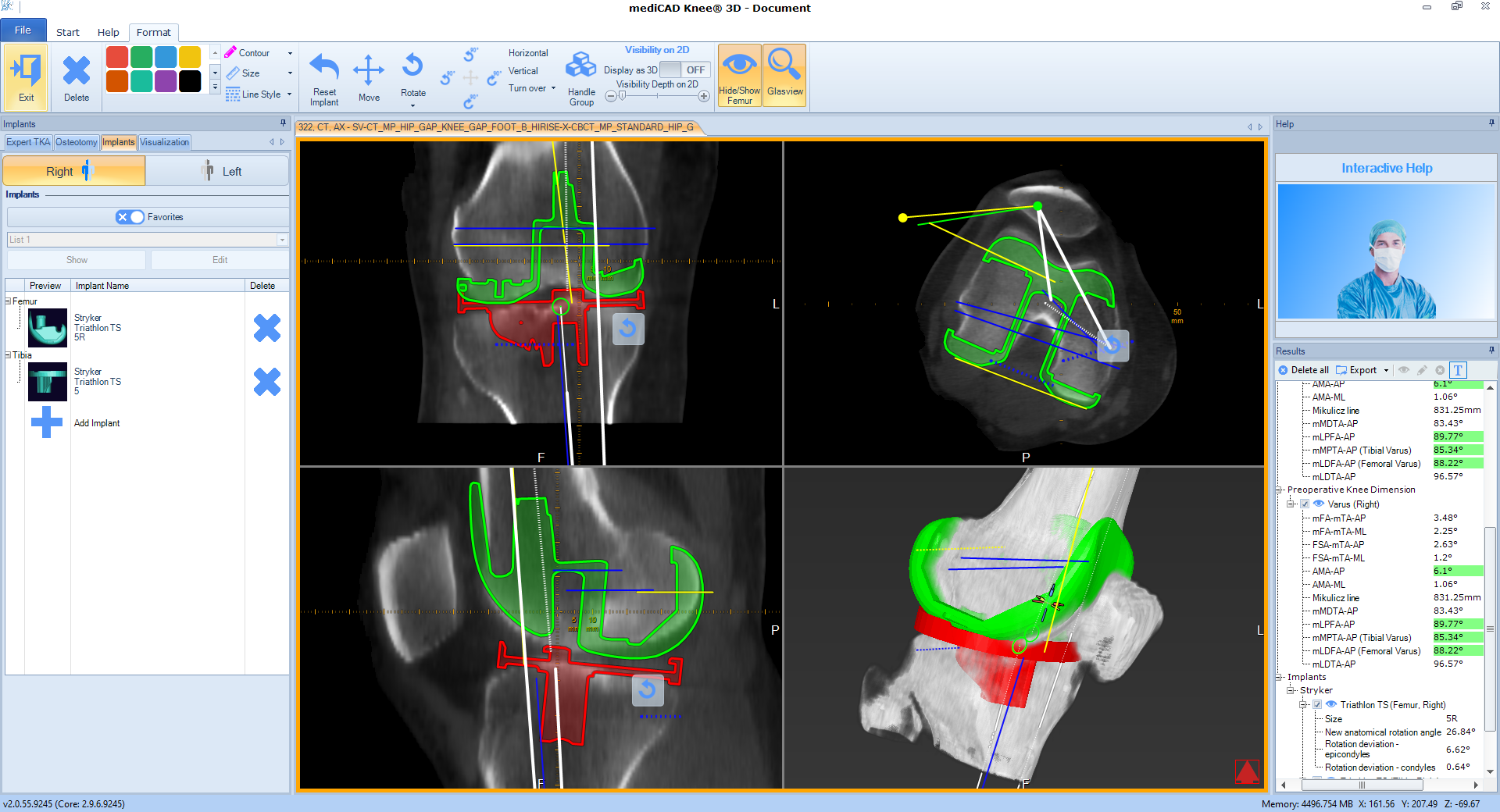
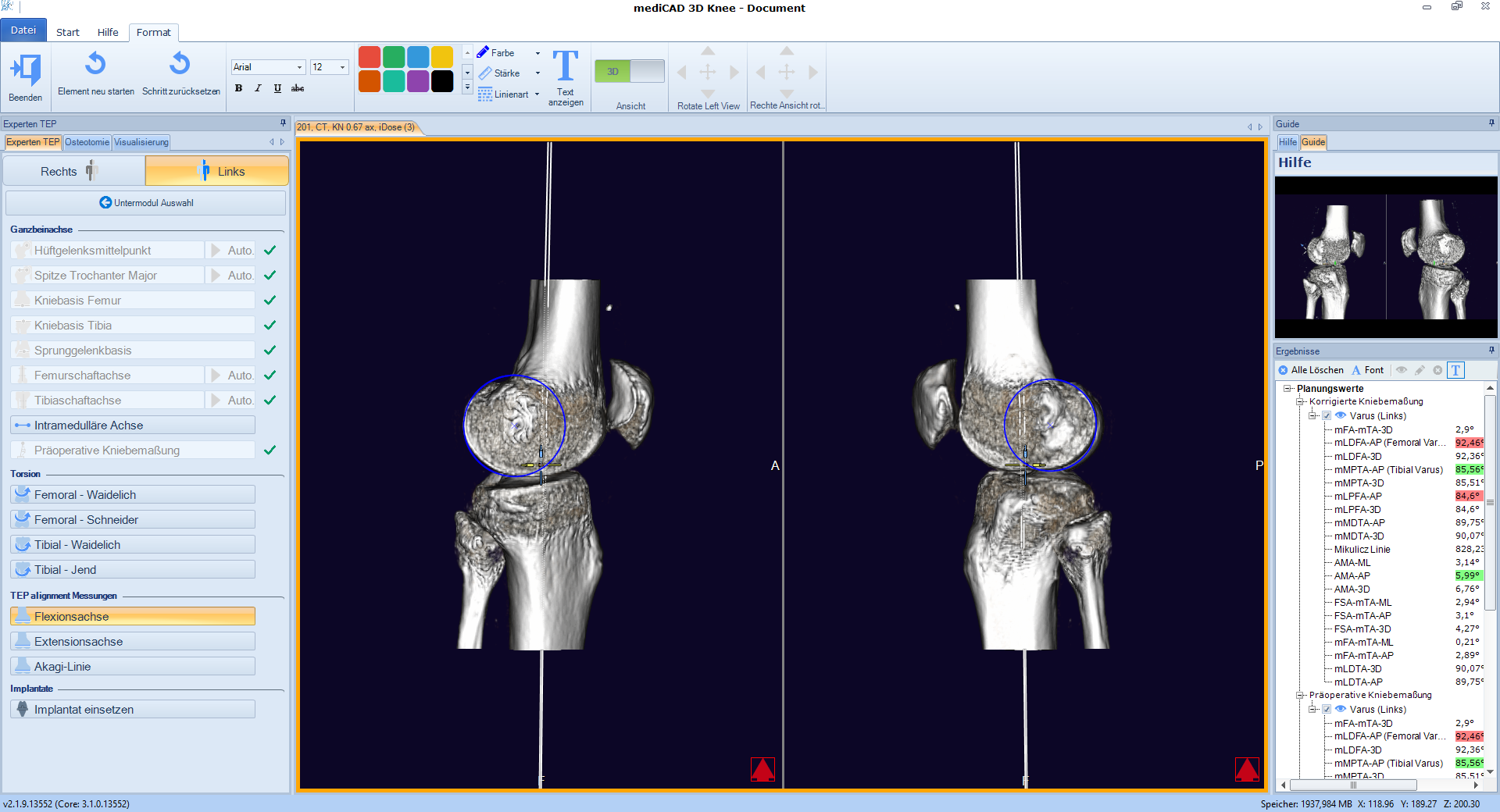
This is possible through a TKA workflow comprising the definition of several important landmarks including the transepicondylar and transcondylar axis as well as a resection on femur and tibia allowing for an oblique joint line or some degrees of Varus/Valgus. All that can be planned on an x-ray and CT or MRI scan. Additionally, patellar height must not be compromised on which is ensured with a thorough assessment of the patellofemoral joint to prevent problems arising from a Patella baja.
3D-planning shall contribute to improve patients’ satisfaction and have the planning performed by the surgeon as each surgeon can perform an individual PSI thanks to 3D-planning.
(mediCAD® recommends the imperial knee protocol for CT scans to ensure a low radiation dose while obtaining a maximum of information).
1)Rivière C, Vigdorchik JM, Vendittoli PA. Mechanical alignment: The end of an era! Orthop Traumatol Surg Res. 2019 Nov;105(7):1223-1226. doi: 10.1016/j.otsr.2019.07.005. Epub 2019 Aug 1. PMID: 31378698.
2)Keshmiri A, Schöttle P, Grifka J, Maderbacher G: The patella in knee replacement. OUP 2017; 6: 328–333 DOI 10.3238/oup.2017.0328–0333
3)Schwick BC, Lehmann W, Baums MH. Femoropatellares Maltracking als Ursache einer schmerzhaften Knieprothese. Knie J. (2020). doi.org/10.1007/s43205-020-00072-x
4)Petersen W, Rembitzki IV, Brüggemann GP, et al. Anterior knee pain after total knee arthroplasty: a narrative review. Int Orthop. 2014;38(2):319-328. doi:10.1007/s00264-013-2081-4
5)Chen Z, Gao Y, Chen S, et al. Biomechanics and wear comparison between mechanical and kinematic alignments in total knee arthroplasty. Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine. 2018;232(12):1209-1218. doi:10.1177/0954411918811855
6)Vanlommel L, Vanlommel J, Claes S et al. Slight undercorrection following total knee arthroplasty results in superior clinical outcomes in varus knees. Knee Surg Sports Traumatol Arthrosc 21, 2325–2330 (2013). doi.org/10.1007/s00167-013-2481-4
7)Hirschmann MT, Becker R, Tandogan R et al.Alignment in TKA: what has been clear is not anymore!. Knee Surg Sports Traumatol Arthrosc27, 2037–2039 (2019). doi.org/10.1007/s00167-019-05558-4
8)Mattei L, Pellegrino P, Calò M, Bistolfi A, Castoldi F. Patient specific instrumentation in total knee arthroplasty: a state of the art. Ann Transl Med. 2016;4(7):126. doi:10.21037/atm.2016.03.33
9)Hirschmann MT, Moser LB, Amsler F, Behrend H, Leclerq V, Hess S. Functional knee phenotypes: a novel classification for phenotyping the coronal lower limb alignment based on the native alignment in young non-osteoarthritic patients. Knee Surg Sports Traumatol Arthrosc. 2019 May;27(5):1394-1402. doi: 10.1007/s00167-019-05509-z. Epub 2019 Apr 11. PMID: 30976825
10)Rivière C, Iranpour F, Auvinet E, Howell S, Vendittoli PA, Cobb J, Parratte S. Alignment options for total knee arthroplasty: A systematic review. Orthop Traumatol Surg Res. 2017 Nov;103(7):1047-1056. doi: 10.1016/j.otsr.2017.07.010. Epub 2017 Aug 31. PMID: 28864235