


When was the last time you consulted a road atlas? Nowadays we use Global Positioning Systems (GPS) for navigation. Similarly, in orthopaedics, more and more surgeons are using specialised 3D-CT software to plan hip and knee arthroplasties, as the benefits of using such systems are becoming more recognised and CT technologies continue to improve. Some examples of commercially available CTbased 3D planning software include ZedHip (LEXI), mediCAD (HecTec), Hip-Plan (Symbios) and Ortoma Plan.
Although CT itself has been used for planning joint replacements for over 30 years [1], preoperative planning with 3D-CT is a more recent concept in orthopaedics. The surgical planning potential of 3D-CT was first explored for craniofacial surgery in the 1980s after it was found that 3D reconstructions could be generated from CT data [2,3].
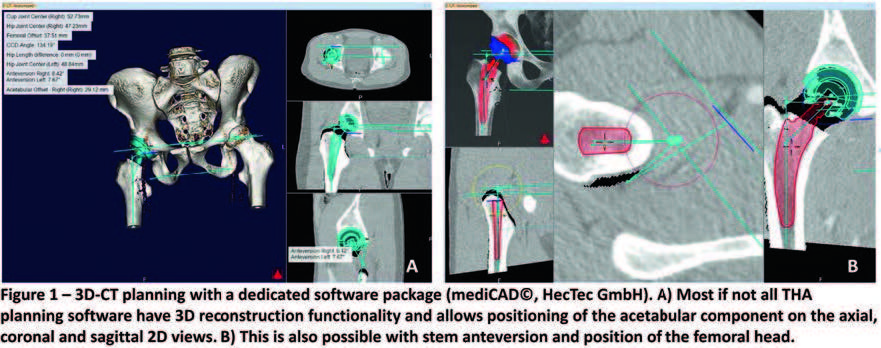
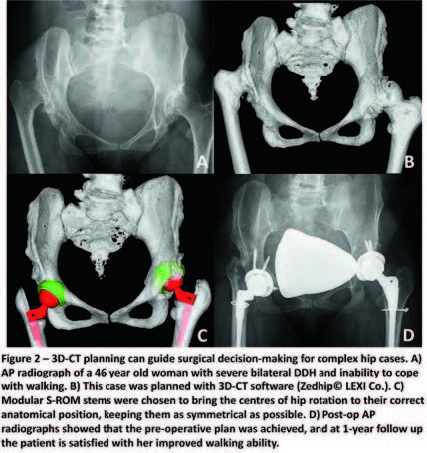
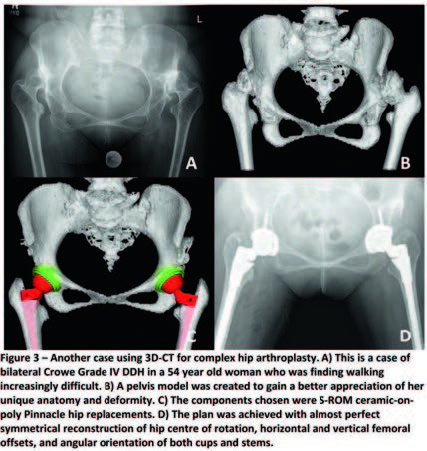
Since then, two main surgical applications of 3D-CT in orthopaedics have been described. The first is 3D printing, where 3D-CT models can be used to create physical models that surgeons can hold in their hands and inspect [4,5]. These models may even be used to simulate surgery and for training purposes. The second is dedicated planning software that surgeons can feed patients’ CT data into and produce detailed 3D-based surgical plans; these computed plans can then be modified and adjusted by surgeons according to what they deem to be best for the individual patient [6,7]. This article will discuss planning software primarily in the context of hip and knee arthroplasties.


As software, the vast majority of 3D-CT planning systems are programmed to run on the Windows operating system. While this normally does not pose a problem due to the ubiquity of Windows, it is still worth considering potential difficulties faced by medical institutions or professionals who prefer other computer operating systems, in which case even less 3D-CT planning software would be available.
Furthermore, there may be compatibility issues with regard to an institution’s CT scanning protocols and those required by some planning software. Often, CT acquisition parameters such as the collimation and type of bone reconstruction kernel must follow specific presets in order to produce scans that can be used with the software. Hence, existing imaging and scanning protocols would need to be reviewed prior to distribution of 3D-CT planning systems throughout an institution.