Lorem ipsum dolor sit amet, consetetur sadipscing elitr, sed diam nonumy eirmod tempor invidunt ut labore et dolore magna aliquyam erat, sed diam voluptua. At vero eos et accusam et justo duo dolores et
Veröffentlicht am, 21.10.2022
In the past preoperative planning on MRIs and CTs were limited to a few cases, e.g., corrections of complex deformities, revision cases, and torsional corrections via a single cut osteotomy. Standard primary arthroplasty cases and corrective osteotomies on the long leg are still commonly planned on an x-ray in AP with the patient being under weight-bearing conditions, i.e., in an upright position.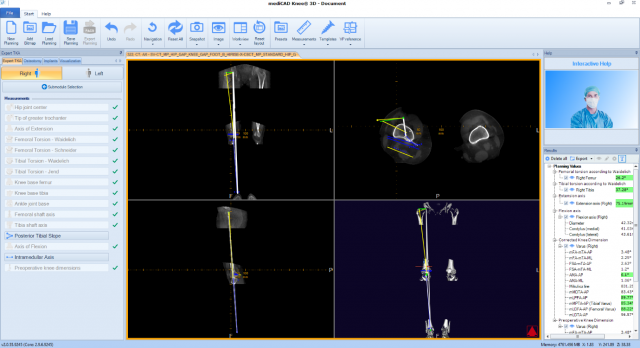
Taking 3D image material, such as an MRI or CT scan for such cases used to be considered not to be justifiable, because the radiation dose of a CT was far too high and scans could only be taken in a supine position of the patient, not in a weight-bearing condition and therefore without considering the band laxities. Both these problems are abandoned by CBCT, the radiation dose is higher than the one of x-rays, though.
A CBCT can be taken on a patient under weight-bearing conditions since the fan beam of a CT has been replaced with a cone- shaped beam, therefore it is called Cone-beam CT. This kind of scanning procedure ensures a fast scan with a low dose because only 3-5 images are required in total to generate the CT-like slice views. This means that a region with a field of view of the pup to 40 cm in height can be scanned in a fracture of the time and radiation dose, but with virtually infinitely thin slice thickness. This comes only at the cost of noise caused by the patients’ movement during the scan. CBCT has for the first time been used in orthopedics for scans of the foot and ankle. 1)
Recently the portfolio is expanding and even whole leg CBCT scans are possible as of now. This offers groundbreaking new options for preoperative planning of any kind of orthopedic surgery, be it an arthroplasty or a corrective osteotomy because it combined 3D image material with the weight-bearing condition, which was for so many years impossible.
Among devices available on the market there are the Planmed Verity and Clarity 2), Curvebeam PedCAT (Foot/Ankle), Line up (Foot to knee) and Hi-Rise (Foot to hip) 3) and the Siemens Multitom Rax 4) which does not only combine an x-ray mode and a CBCT mode but can as well take CBCT scans in a supine and in a weight-bearing position. With NewTom 5) there is as well a manufacturer of supine state CBCTs, e.g., for the shoulder and the upper extremities in general.
The diagnosis of arthritis of the knee, as well as the surgical plan and its accuracy can be much improved by applying only a bit more radiation, which justifies taking this kind of image material a lot more than taking an ordinary CT.
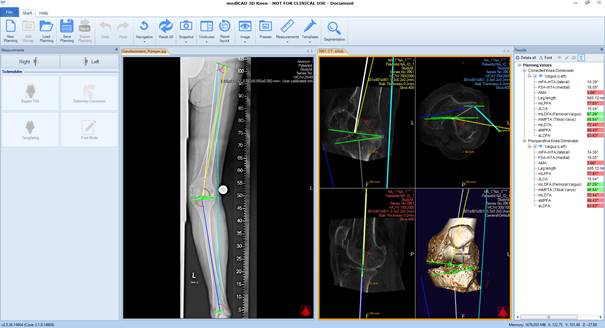
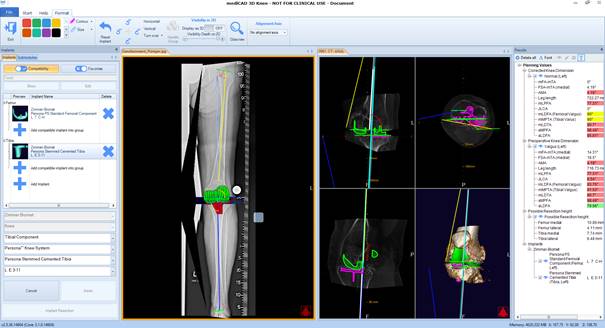
Possible use cases can be planning on a weight-bearing frontal x-ray in combination with a CBCT scan of the knee to plan the correction and resection on the x-ray and determine the size and rotation, as well as flexion and Varus/Valgus positioning on the CBCT. For the planning of a corrective osteotomy, it is especially the change in tibial slope being affected by an HTO, the torsion, and the patella tracking which can be enlightened when planning on a torsional profile protocol in the weight-bearing position as taken by such devices. Single cut osteotomies become much less of a challenge because they, too, can be planned like that, having full control of the preoperatively defined values.
Therefore, mediCAD strongly encourages the use of our 3D planning tools in combination with CBCT devices. Image material has been widely tested to be compatible with mediCAD 3D software solutions.